Burkitt Lymphoma
a form of non-Hodgkin's lymphoma
Associated with Epstein Barr Virus and is commonly located in the
jaw of Africans (the classic patient)
Classic Translocation = t(8;14) which moves the c-myc gene on chromosome 8 right next to the Immunoglobulin (Ig) Heavy Chain.
Here is a joke for you. I hope you find it hilarious. Okay, a giggle will do. Tell it to someone else, embrace the awkwardness that ensues and that should tattoo it to your brain for a while.
How come Mick ate one for?-----Here is what the joke really means----
come Mick = c-myc
ate = 8 - since c-myc is on chromosome 8
one = 1
for = 4
To get heavy!heavy = Ig Heavy chain which is on chromosome 14
And here's a little doodle to drive it on home:

That big guy there is Mick (myc) who has just ate (8) one (1). For (4) what? To get heavy.
c-myc is on chromosome 8
Ig Heavy chain is on chromosome 14
Believe me, this joke is much funnier if you're telling it to yourself when you are looking at a question on it.
Here is what some practice questions I've seen ask and is mentioned in various review therefore I made sure I knew this for my exam although I had to look it up again for this post.
The function of c-myc: c-myc is a
proto-oncogene which codes a protein that regulates
nuclear transcription. When it is moved next to the gene for the Ig heavy chain it becomes constantly active since the body is constantly making Ig heavy chains. At this point it is now called an
oncogene. c-myc now causes the B-cells to constantly reproduce themselves over and over again. This results in a
high grade lymphomaThis is in contrast to
B-cell follicular lymphomas in which BCL-2 (a gene which promotes apoptosis). When BCL-2, a tumor suppressor gene, is translocated it becomes functionally inactive and so B-cells can't undergo apoptosis the same anymore. This is an example of low grade tumor.
So I think this is how you should think about it: Burkitt's lymphoma is when B-cells actively divide whereas in B-cell follicular lymphomas, B-cells don't die.
Also, here's the classic"Starry Sky Appearance"
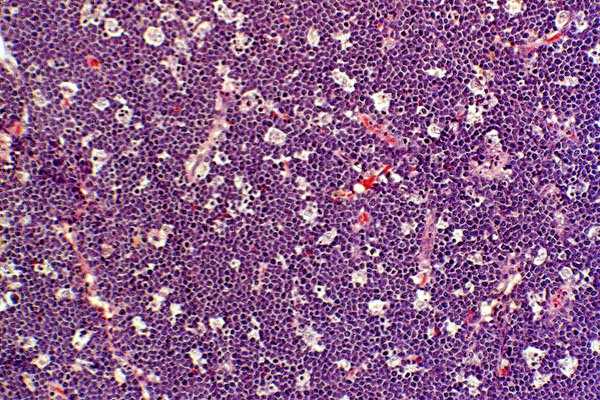
I just want to point out here what that refers to. The dark purple areas are really just a bunch of neoplastic B-cells that are dividing much more rapidly now that c-myc is always active. ("Dark is Dividing") The stars are the lighter areas which are much fewer in number - these are the macrophages. I'm not sure what they are doing there, but I do know that they are NOT the problem. Perhaps they are trying to help out in getting rid of the tumor.
That's what I think is really important for this tumor that seems to be a pretty hot topic for the exam.













